Patient initially sustained a periprosthetic distal femur fracture which was repaired at another hospital.Over time the fi xation failed, and the reduction was lost, resulting in the development of a varusdeformity. The patient was referred for re-construction. The initial fi xation was removed, themalalignment was corrected, and the metaphysis was impacted into the proximal segment to gainstability and alignment.
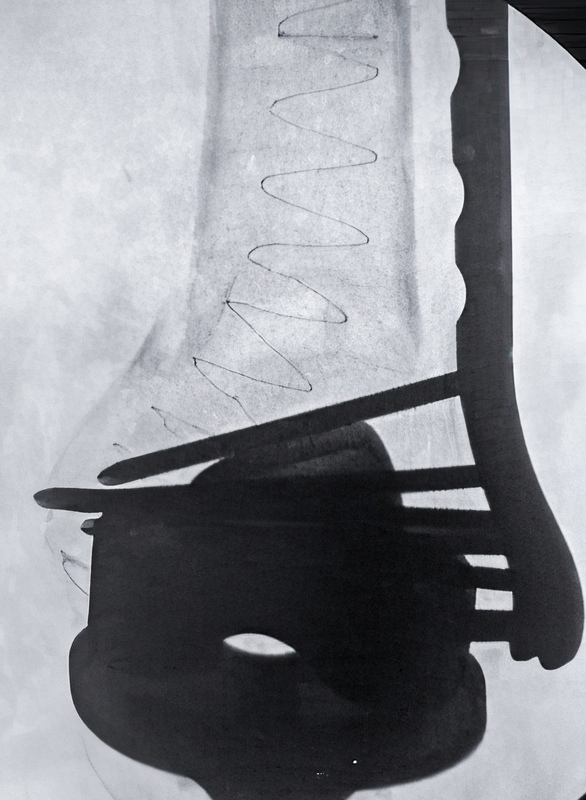
A supracondylar variable angle locking plate was inserted utilizing minimally invasive techniquespositioned on the lateral cortex and provisionally fi xed with k wires. The plate was secured and thereduction maintained with anterior based locking screws in the femoral condyles and blunt unicorticalscrews proximally, to avoid penetrating the intramedullary canal. A percutaneous approach was madeto the distal most aspect of the medial femoral condyle in line with the IM canal on lateral imaging. Acannulated awl was used to gain access to the intramedullary canal adjacent to the femoral component.A guide wire was placed in the IM canal and across the fracture site, and the canal was reamed to clearthe canal and to accept the IlluminOss sheath. An IlluminOss implant was inserted. Its length waschosen to be shorter than the plate length avoiding a proximal stress riser. On X-ray, there was nointerference with the IlluminOss implant from the screw fi xation through the lateral plate. Once theimplant was fi lled appropriately with photodynamic liquid monomer, it was cured with visible bluelight. Enhanced screw fi xation was achieved by placing both variable angle locking screws distally andbicortical screws proximally into the IlluminOss implant, augmenting fracture stabilization. Patient wasplaced in a soft dressing with no motion restrictions and was encouraged to begin immediate weightbearing as tolerated.